Author: Alec Furstenberg, MD, Emergency Medicine Resident, PGY1
Faculty: Alexis Cates, DO, Medical Toxicology/Emergency Medicine Attending
The Case:
A 67 year old woman with past medical history of atrial fibrillation on warfarin, Type II diabetes mellitus, hyperlipidemia and hypertension presents to a large, urban emergency department with EMS after being found down by her husband. Per the husband, the patient was in her usual state of health when he left for a business trip Friday morning. He returned Monday morning and found her slumped on the couch, covered in urine and feces. The patient was obtunded and actively vomiting, unable to provide further history. She was intubated for airway protection due to her depressed mental status and active vomiting.
Past medical history: as above
Medications: Metformin 500 mg BID, Atorvastatin 40 mg qd, losartan 100 mg qd, amlodipine 10 mg qd, HCTZ 25 mg BID, ASA 81 mg qd, Warfarin 5 mg qd, Tylenol 500 mg PRN
Allergies: NKDA
Surgical history: None
Social: 1-2 drinks per week, no tobacco use, no recreational drug use
Vitals: T 37.0C, BP 210/98, HR 51, RR 27, SpO2 98% on room air
Learning point 1: Warfarin Toxicity

Figure 1: Coagulation cascade demonstrating how different anticoagulants can enact effects
Warfarin toxicity presents a unique challenge for providers. There isn’t a classic toxidrome. It may present as simply and benignly as epistaxis or gingival bleeding after brushing teeth to as severely as seen in this patient- complete obtundation due to a critical bleeding scenario. There are three main mechanisms in which warfarin toxicity occurs: intentional adult overdose, unintentional overdose/secondary toxicity due to metabolic issues, and pediatric exploratory ingestion. Unintentional toxicities are the most commonly seen, accounting for around 84% of all cases on a yearly basis1.

Figure 2: Warfarin’s mechanism of action
As outlined in the coagulation cascade, warfarin inhibits the vitamin K-dependent factors. It does so by inhibiting vitamin K epoxide reductase, which prevents reduction of vitamin K into its active form. The factors are II, VII, IX, and X.

Figure 3: Warfarin metabolism in the liver
Warfarin is metabolized by the CYP450 enzyme system, mostly CYP2C9. As such, it is subject to metabolic changes based on other things that induce or inhibit these enzymes. Some of the common inducers that may result in a hypercoagulable state include phenytoin, rifampin, carbamazepine, and St. John’s wort2. On the other end, commonly offending inhibitors of CYP2C9 include amiodarone, fluoroquinolones, clarithromycin, azoles, isoniazid, ritonavir, and trimethoprim/sulfamethoxazole. Trimethoprim/sulfamethoxazole does so by inhibiting CYP2C9, which as demonstrated in Figure 3, helps metabolize the S-enantiomer of warfarin, the predominant form seen in patients3. This inhibition leads to accumulation of warfarin in the blood and thus unregulated blockage of the coagulation cascade.
Learning Point 2: Evaluation of suspected warfarin toxicity
It can be rare that a provider starts a workup for suspected warfarin toxicity. Rather, the clinical vignette often presents a patient with a downstream event: hematuria, hemarthrosis, or intracranial hemorrhage resulting in altered mental status. In this case, the presenting symptom was altered mental status (AMS). As such, a broad workup – especially in an elderly patient – is warranted for further evaluation of their mental status change.
- Point-of-care glucose
- A quick, cheap test that provides you information on whether the patient requires immediate intervention
- Venous blood gas
- To provide acid/base status and screening lactate
- Complete metabolic panel
- To evaluate renal function, electrolyte status and liver function tests
- Coagulation studies
- To evaluate for synthetic liver dysfunction
- To determine whether patient is therapeutic on warfarin dose
- Troponin
- If there is concern for cardiac ischemia
- Pregnancy test
- When of child-bearing age
- Urinalysis
- To determine if hematuria exists or concomitant urinary tract infection
- Urine drug screen
- To evaluate for incidental or intentional exposure to commonly tested illicit substances
- Alcohol level
- Can cause AMS with anion gap metabolic acidosis
- Acetaminophen/Salicylate levels
- Patients often coingest these when uncomfortable at home or with intentional ingestions
- EKG
- Identify dysrhythmias that could be primary or secondary to electrolyte derangements in an altered patient
- Chest X-Ray
- Pneumonia or other thoracic pathology may contribute to changes in mental status
- CT Head
- Especially in first time or new-onset AMS
Learning Point 3: Management of warfarin toxicity
Following usual resuscitative measures, the first step in suspected warfarin toxicity is to hold the patient’s warfarin. The next step is to decide on the urgency of anticoagulation reversal. If the patient is asymptomatic or has only mild symptoms – controlled epistaxis or gingival bleeding – it is appropriate to administer PO vitamin K as the sole intervention, with a dose-dependent relationship on the INR.
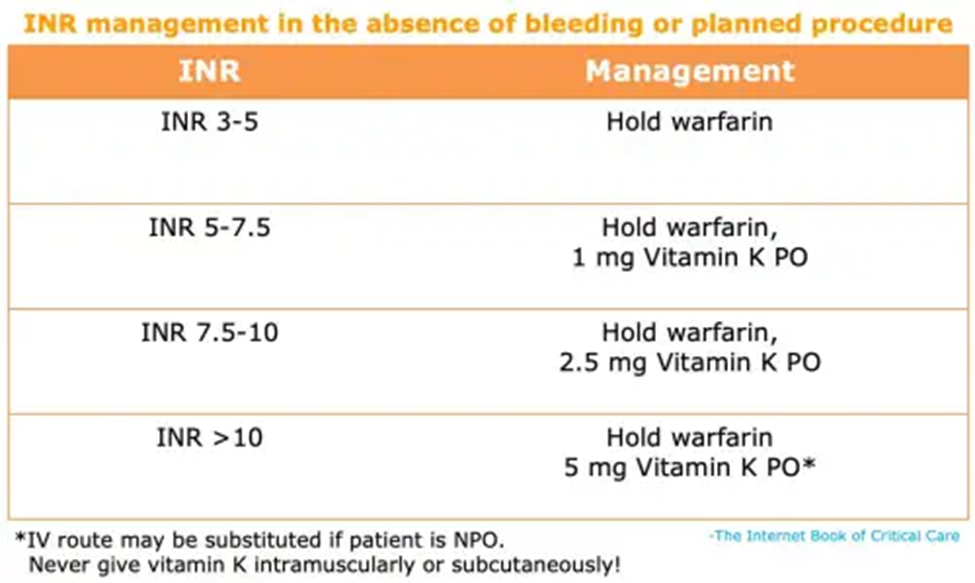
Figure 4: PO Vitamin K guidelines for warfarin toxicity
For emergent warfarin reversal, particularly in a critically ill patient with significant bleeding, the vitamin K must be administered intravenously, and should be done so at a dose of 10 mg infused over 30 minutes4. The patient should concurrently receive 1500 units of IV prothrombin complex concentrate (PCC), though one can consider 50 units/kg PCC with a max dose of 5000 units if there is intracranial bleeding with an INR > 6, as was suspected in this case. It is important to co-administer these reversal agents as PCC works for approximately 8 hours and IV vitamin K takes approximately 6-12 hours to take effect.
The Case Continued…
This patient’s initial POC glucose was 171and VBG returned with a pH of 7.18 and pCO2 of 42 with a lactate of 4.21. Given she was actively vomiting in the room and altered, she was intubated for airway protection and taken for CT head without contrast expeditiously. There, she was found to have a large, acute intracranial hemorrhage with 3 mm of midline shift. Neurosurgery was paged and the ED team was made aware of plans for decompressive hemicraniectomy.
While the ED team had an explanation for the patient’s altered mental status at this time, there still wasn’t a strong explanation for the etiology. Labs returned as follows:
- CBC
WBC 9.8×10^3/L
Hgb 12.1 g/L
Plt 324,000/L - BMP with Mg/PO4
Na 139 mm/L
K 4.6 mm/L
Cl 102 mm/L
HCO3 42 mm/L
BUN 33 mg/dL
Cr 1.41 mg/dL
Mg 1.7 mg/dL
PO4 3.2 mg/dL
- LFTs
Alkaline Phosphatase 170 IU/L
AST 68 IU/L
ALT 72 IU/L
PT: 39s
PTT: 46s
INR: 8.1
Troponin WNL
- EKG
Atrial fibrillation at a rate of 55 beats per minute
No T-wave inversions or ST changes - Alcohol/Acetaminophen/Salicylate levels undetectable
- Urinalysis was negative for blood, bacteria, LE, and nitrites
- Blood/Urine cultures had no growth at 4 days
- Chest Xray negative for infection or acute cardiopulmonary disease
You notice the PT/INR are significantly elevated, indicating that the patient is supratherapeutic with her warfarin. What happened?
Learning Point 4: Medication interactions
When paired with the patient’s altered mental status, hypertension, and bradycardia, the finding of her intracranial hemorrhage points towards supratherapeutic warfarin dosing as the culprit for her clinical picture. However, 5 mg of warfarin per day had been this patient’s dose for over 10 years, per her husband. What changed?
In a review of her external prescriptions, it was learned the patient had filled a 7-day course of trimethoprim/sulfamethoxazole written by her out-of-network primary physician on Friday morning. The inpatient team called the primary physician and discovered the patient had a urine dipstick positive for leukocyte esterase and nitrites on Thursday with a culture that eventually grew pan-sensitive E. coli. He prescribed 1 double-strength tablet of trimethoprim/sulfamethoxazole every 12 hours for her urinary tract infection. The physician failed to recognize how adding this medication could create catastrophic polypharmacy. As previously outlined, trimethoprim/sulfamethoxazole inhibits CYP2C9 which leads to warfarin buildup due to lack of metabolism and inhibition of coagulation.
While there was no second-hand account of this patient’s deterioration, it was assumed that her compliance with both trimethoprim/sulfamethoxazole and warfarin caused a drug-drug interaction. Trimethoprim/sulfamethoxazole inactivated CYP2C9, which resulted in supratherapeutic warfarin levels. Perhaps the patient became progressively altered, either from her urinary tract infection or from an expanding intracranial hemorrhage, and became medication noncompliant, resulting in worsening hypertensive crisis and intraparenchymal hemorrhage.
The Case Concluded…
Prior to surgery, the patient was given 10 mg of IV vitamin K and 4500 units of prothrombin complex concentrate (PCC). She was taken for decompressive hemicraniectomy and did well postoperatively. Her warfarin was held for the next several days and her trimethoprim/sulfamethoxazole was switched to cephalexin. Her repeat CT of her head showed improvement of midline shift and no further bleeding. Over the next several days, her INR normalized to 2.6 and she resumed 5 mg of warfarin daily while being monitored for three additional days for INR checks.
References
1. Justin, Deaton G, and Thomas M Nappe. “Warfarin Toxicity – Statpearls – NCBI Bookshelf.” StatPearls, Treasure Island, 21 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK431112/.
2. Lynch, Tom, and Amy Price Neff. “The Effect of Cytochrome P450 Metabolism on Drug Response, Interactions, and Adverse Effects.” American Family Physician, American Association of Family Physicians, 1 Aug. 2007, https://www.aafp.org/afp/2007/0801/p391.html.
3. Busti, Anthony J. “The Mechanism for Trimethoprim/Sulfamethoxazole’s (Bactrim; Bactrim DS; Septra) Inhibition of Warfarin (Coumadin; Jantoven).” EBM Consult, Aug. 2015, https://www.ebmconsult.com/articles/tmp-smx-bactrim-septra-warfarin-coumadin-interaction-mechanims.
4. Farkas, Josh. “Anticoagulant Reversal.” EMCrit Project, 8 Dec. 2021, https://emcrit.org/ibcc/reverse/#warfarin:_urgent_reversal.
