Toxicology Talks with Toxijawn
Author: Melissa Yu, DO, Emergency Medicine Resident PGY2
Fellow: Alexis Cates, DO, Medical Toxicology Fellow PGY6
Faculty: James Krueger, MD, Medical Toxicology / Emergency Medicine attending
The case.
A 28 year old female presents to the ED for evaluation of a bump to the left arm that she thinks started as a bug bite a few days ago while she was vacationing far away in Vietnam. It is pruritic, painful, erythematous and exhibits purulent discharge. She states that she has a history of methicillin-resistant staphylococcus aureus infections (MRSA) in the past. She is afebrile. You start writing her discharge paperwork and prepare a prescription for trimethoprim-sulfamethoxazole, an antibiotic with MRSA coverage, when your attending reminds you that your patient is of child-bearing age. You get a pregnancy test and it is positive.
Learning Point 1: Don’t forget the HCG!
When treating a person of child-bearing age, it is important to confirm their pregnancy status. Many xenobiotics (or an agent that is foreign to the human body) can be teratogenic, or an agent that can disturb the development of an embryo or a fetus.
Learning Point 2: Principles of xenobiotics in pregnancy
Xenobiotics can have harmful effects in pregnancy including teratogenicity and intrauterine growth restriction. The basic premise of teratogenicity is that the particular toxic effects of a certain drug are determined by the stage of development of the fetus when the xenobiotic is given, as well as how much of it is given. A general timeline includes:
- Pre-implantation (Weeks 1-2)
- Prior to week 2, exposure to a teratogen produces an all-or-none effect (fetus either survives or does not survive)
- Organogenesis (Weeks 2-15)
- Classic teratogenic period
- Heart & extremities form earlier
- Urinary system forms later
- CNS forms throughout entire pregnancy
- Fetal growth (Weeks 15+)
When considering xenobiotics for pregnant females, it is also important to understand the physiologic changes in a pregnant woman, which can affect the efficacy and therapeutic dosing.
- Factors that can increase xenobiotic concentrations in the body
- Delayed gastric emptying –> more complete GI absorption & lower peak plasma concentrations
- Increased blood flow to skin & mucous membranes –> increased dermal and mucosal absorption
- Increased tidal volume and decreased residual lung volumes –> increased inhalation exposure
- Decreased plasma albumin and decreased hepatic biotransformation late in pregnancy –> increased free (unbound) xenobiotic
- Factors that can decrease xenobiotic concentrations in the body
- Increased fat stores, plasma & ECF volume early in pregnancy –> greater volume of distribution –> less free xenobiotics
- Increased GFR –> increased renal excretion
Learning Point 3: Know common teratogens & prescribing resources
Unfortunately, one of the frustrations of prescribing xenobiotic therapy in pregnancy is the unknown. There are some medications that have been tested in humans and found to either cause or not cause harm; however, the reality is that for most xenobiotics, there is little to no information, or even conflicting information, on actual human studies.
Previously, the Food and Drug Administration (FDA) had listed 5 categories of labeling for drug use in pregnancy, (what most of us know as A, B, C, D, X). In 2015, it has been gradually shifting towards a new labeling system called the PLLR, or “Pregnancy and Lactation Labeling Rule.” Concerns regarding the prior labeling system were that it did not accurately communicate differences in the degree of fetal risk, resulting in frequent misinterpretation of the labeling system by physicians. The new PLLR system requires drug companies to provide specific summaries of risks, discussion on human and animal data, as well as specific considerations to help physicians and other health care providers make prescribing decisions.
Here is a list of commonly tested xenobiotics that are known to be teratogenic:
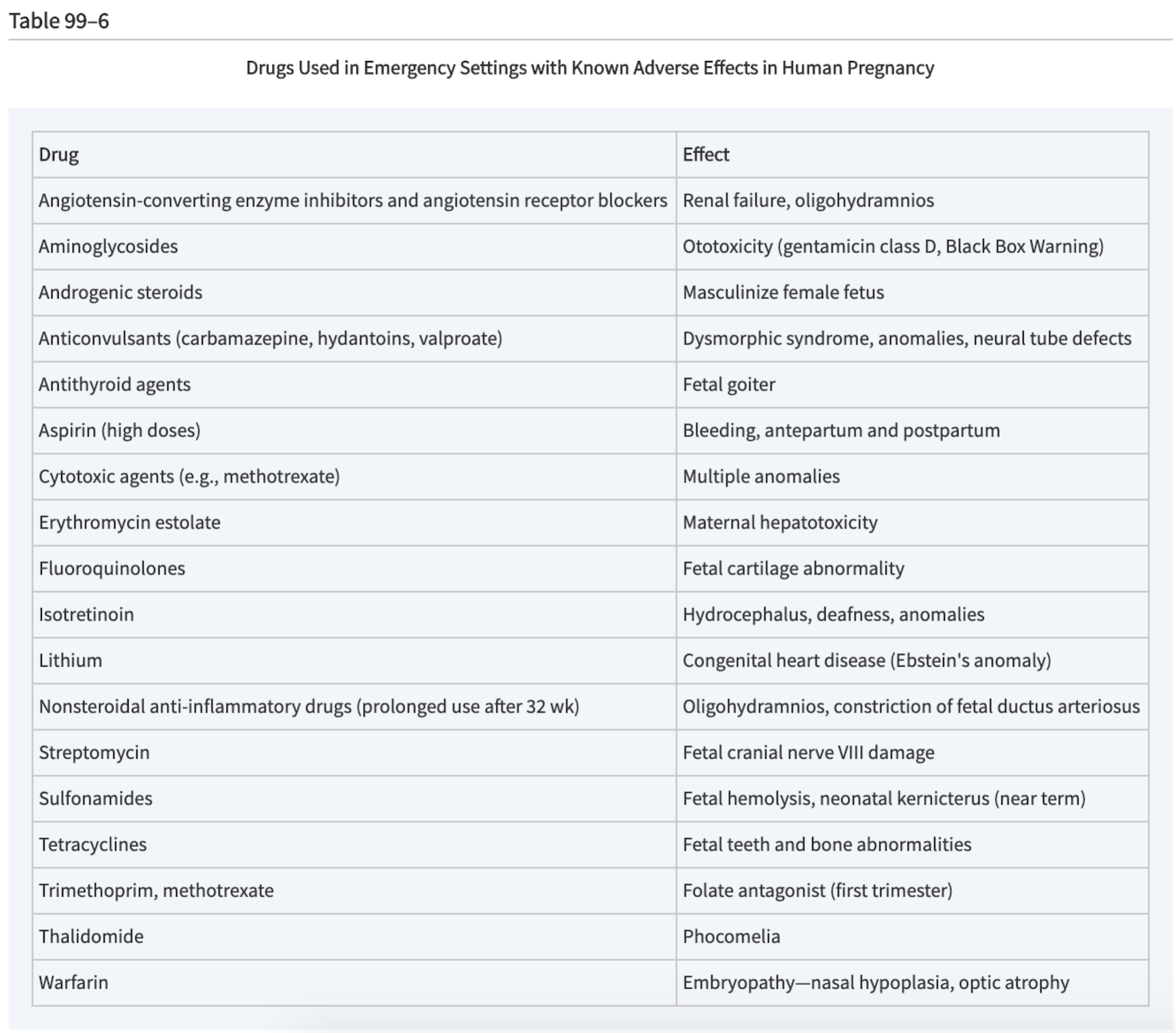
Source: Tintinalli’s Emergency Medicine, 8th Edition
After doing some research, you decide to write a prescription for clindamycin instead of trimethoprim-sulfamethoxazole for your patient. When you go into the room, you note that she looks slightly tachypneic. She states that she started feeling short of breath while in the emergency department. Her lungs are clear, and she remains afebrile. She has sinus tachycardia on an EKG and on the cardiac monitor at bedside. You remember that she recently returned on a long flight from Vietnam. In addition to pregnancy, you note that this prolonged stasis is a risk factor, and you become concerned that she may have developed a pulmonary embolism. You question what kind of imaging is best for the patient at this unknown stage of gestational development.
Learning Point 4: Fetal radiation effects
When obtaining radiology studies on pregnant patients, one must always weigh the risk of fetal exposure against the risk of incorrect maternal diagnosis. When radiology is needed, always follow the ALARA (As Low as Reasonably Achievable) principle. The biggest factor in determining the degree of risk to the fetus is the amount of ionizing radiation exposure, and the age of gestation when exposed. The general radiation exposure that is accepted as safe in pregnancy is <50mGy. Below is a table from Tintinalli’s Emergency Medicine highlighting different procedures and their radiation exposure to the fetus:
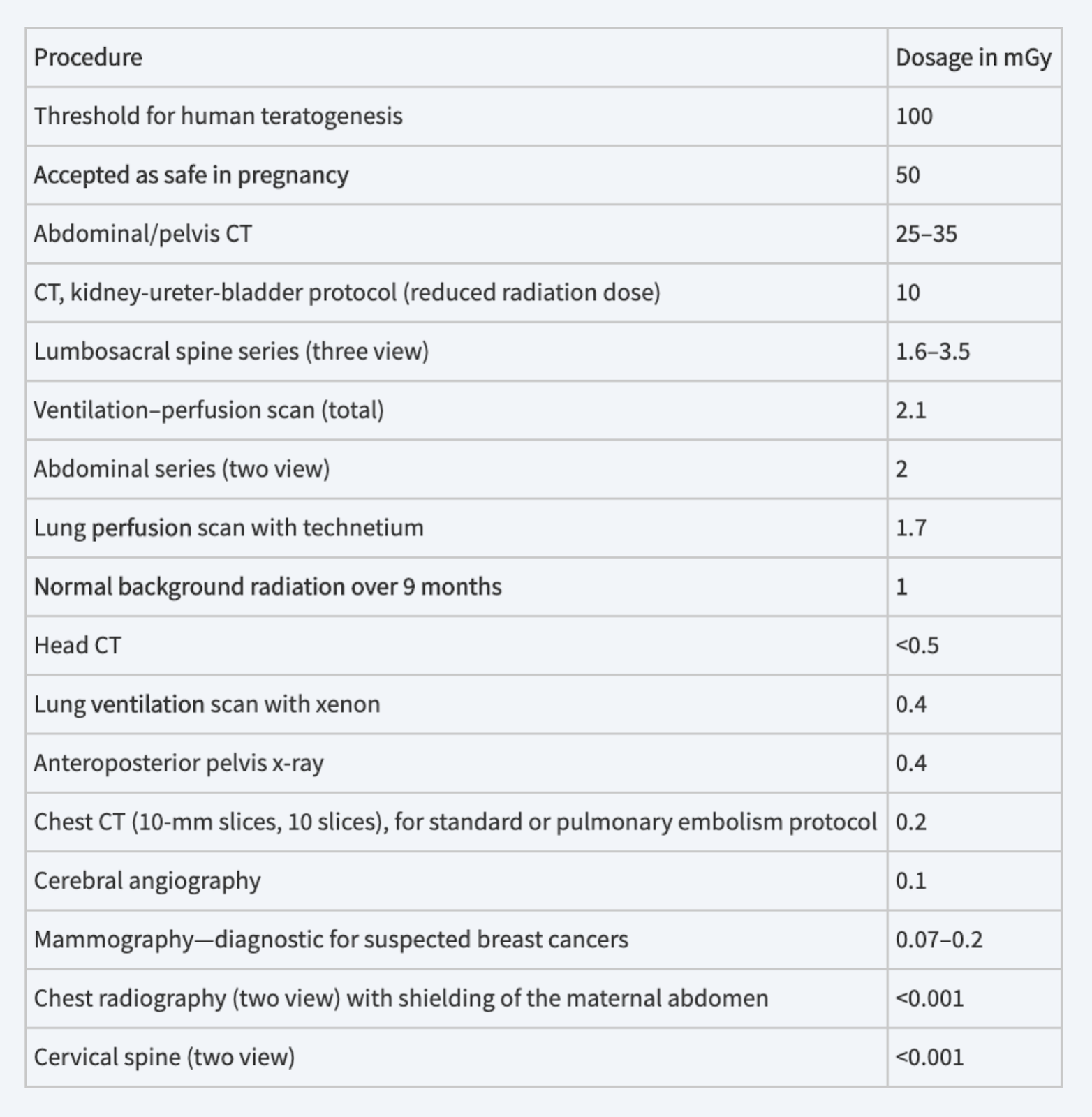
Source: Tintinalli’s Emergency Medicine, 8th Edition
You begin with a chest x-ray, and interpret it as normal. You then follow this study with a computed tomography scan with an angiogram of the chest which confirms the diagnosis of pulmonary embolism. Her blood pressure is normal, but she remains somewhat tachypneic and tachycardic. The patient is started on low molecular weight heparin. You order an ultrasound to evaluate the fetus and admit the patient for monitoring with obstetric consultation.
Learning Point 5: A sick mom is a sick baby!
In an emergent situation, the priority should be to treat the mother, which would ultimately treat the baby. One should consider FDA guidelines for xenobiotics and fetal radiation concerns as mentioned before, but if the mother is sick, then the baby is likely also sick. It is essential to ensure appropriate treatment for the condition you suspect in the mother, and get consultants on board early, as needed.
Online resources to check out:
- EMDocs article on safe medications during pregnancy
- Information from the FDA on medications
- Fact sheets for parents on “Mother To Baby”
- LactMed Internet Database with information on xenobiotics in lactation
