Author: Alexander Busch, DO, Emergency Medicine Resident PGY1
Fellow: Richard Chen, MD, Medical Toxicology Fellow PGY5
Faculty: James Krueger, MD, Medical Toxicology / Emergency Medicine Attending
The Case:
You are a resident working in a level 1 trauma center. A 62 y/o female presents to the ED after a fall. Initial workup shows no injury aside from a 5 cm laceration to the right forearm. You offer to allow the new medical student rotating in the department to suture the wound. As he enthusiastically agrees, you are asked to see another patient urgently. You tell the student to ask the nurse for 2 bottles of 2% lidocaine and instruct him to get you once he has anesthetized the area, and you will supervise him performing the procedure. About 15 minutes later, the student emerges frantically from the room and tells you that the patient has suddenly become agitated while he was preparing for the procedure. As you enter the room, you notice that the patient’s blood pressure is now 180/110 and her heart rate is now 130. You also notice some significant bleeding from an injection site near the wound and that both 30 mL bottles of lidocaine are empty…
Learning point 1: Recognizing Local Anesthetic Toxicity
- Local anesthetics act through sodium channel blockade of nerve cells when administered locally.
- When administered systemically, either intentionally or inadvertently, sodium channel blockade of CNS nerve cells and cardiac causing neurotoxicity and cardiotoxicity.
- Lidocaine is a commonly used Class IB antiarrhythmic in addition to a local anesthetic.
- Can occur after inadvertent IV injection of local anesthetic or infiltration of large amounts of local anesthetic into the subcutaneous tissue
- More rarely can occur with topical application.
- Toxic doses vary by agent and formulation
- Lidocaine is toxic at 4.5 mg/kg without epinephrine, 7 mg/kg with epinephrine
- Bupivacaine is toxic at 2.5 mg/kg without epinephrine, 3 mg/kg with epinephrine
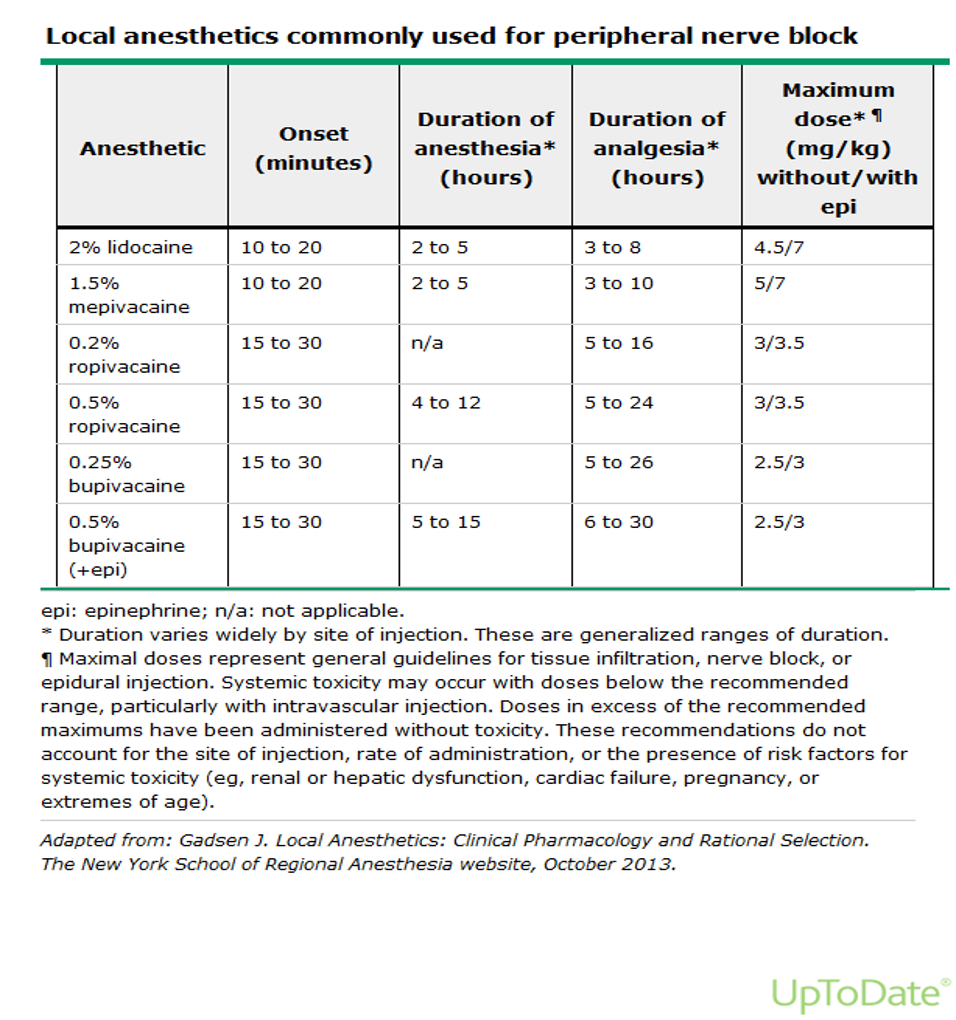
Source: UpToDate “Local Anesthetic Toxicity” Table 3
- Calculation of lidocaine dose:
- Determine concentration of lidocaine solution, typically 1% or 2%
- Concentration is typically represented by grams/100 mL
- This means that 1gm lidocaine/100mL = 1% lidocaine = 10 mg lidocaine/1 mL
- To obtain mg of drug given, multiply amount in mL
- 10cc of 1% lidocaine = 100 mg lidocaine
- Clinical Presentation
- Toxicity develops quickly (10-30 mins) after administration
- Begins with CNS excitation, can progress to inhibition if severe enough toxicity
- Cardiotoxicity and excitation tend to occur after CNS symptoms. Inhibitory cardiovascular symptoms may be present and may lead to cardiac arrest. In bupivacaine toxicity in particular, or in large lidocaine overdoses, patients can progress to cardiotoxicity without symptoms of neurotoxicity.
Neurotoxicity
- Excitation
- Perioral numbness
- Metallic taste
- Mental status change
- Vision changes
- Muscle spasm
- Vertigo
- Seizures
- Depression
- Somnolence
- Respiratory depression
- Coma
Cardiotoxicity
- Often starts with tachycardia and hypertension
- May start with bradycardia and hypotension
- Can progress to ventricular dysrhythmia and cardiac arrest
The case continued.
Having recognized the symptoms of early local anesthetic toxicity, you quickly apologize to the student for not providing better instructions and supervision. You then run out to inform your attending and initiate treatment before symptoms progress.
Learning Point 2: Treating Local Anesthetic Toxicity
- ABCs
- Ensure airway protection
- Use pulse oximetry to evaluate oxygenation
- Intubate and ventilate the patient when necessary
- Attach the patient to a cardiac monitor
- If the patient is hypotensive, consider IV fluid resuscitation with normal saline or lactated ringer’s solution
- Address seizures
- Consider the use of benzodiazepines when indicated, such as:
- Midazolam 1 to 2 mg IV, OR
- Ativan 2 to 4 mg IV
- Consider the use of benzodiazepines when indicated, such as:
- Address dysrhythmias
- Consider the use of other antidysrhythmics when indicated, such as:
- Amiodarone 150mg – 300mg IV
- Consider the use of other antidysrhythmics when indicated, such as:
- Lipid emulsion therapy
- 20% Intralipid
- Dosing based on ideal body weight, not actual body weight
- If patient less than 70 kg, 1.5 mL/kg IV bolus, with infusion after of 0.25 mL/kg/minute
- If patient over 70 kg, then 100 mL IV bolus, with infusion of 200 to 250 mL over 15-20 minutes
- Repeat bolus if cardiovascular instability persists
- Acts as a “lipid sink”, into which excess local anesthetic can distribute, decreasing the active xenobiotic in the serum
- Side effects can result from deposition of lipids into different areas, such as:
- Clots in dialysis catheters or ECMO lines
- DVT
- Pancreatitis
- Lab abnormalities from increased lipids in the serum
- Can decrease reliability of serum drug level measurements
- Measurements of endogenous substances is also affected, most notably:
- AST and ALT
- Bilirubin
- Glucose
- D-dimer
- Lactate
- Lipase
- CK
- Troponin T
- Iron
- When the above does not work, such as in extremely severe cases, ECMO or other cardiac bypass may be needed until local anesthetic is metabolized and dissociates from cardiac myocytes
The case continued.
After stabilizing the patient, you decide to debrief the medical student and use the time as a learning opportunity to teach him methods to prevent local anesthetic toxicity.
Learning Point 3: Preventing Local Anesthetic Toxicity
- Know the maximum dose of the local anesthetic you are using
- Aspirate before injecting local anesthetic; blood return may indicate inadvertent intravascular penetration
- Use small doses divided in space and time
- Ask patient about symptoms during and after administration
- Specify “does this feel sharp” versus “do you feel pressure” when assessing efficacy of given anesthetic
- Patients will continue to feel pressure, but should not feel sharp pain when dose is effective
- Use ultrasound guidance for nerve blocks
Resources:
UpToDate: Local Anesthetic Toxicity
Life in the Fastlane: Local Anesthetic Toxicity
ACMT Toxicology Visual Pearls: The Blood Sample Doesn’t Look Right
Ami M. Grunbaum, Brian M. Gilfix, Robert S. Hoffman, Valéry Lavergne, Martin Morris, Andrea Miller-Nesbitt & Sophie Gosselin (2016) “Review of the effect of intravenous lipid emulsion on laboratory analyses”, Clinical Toxicology, 54:2, 92-102, DOI: 10.3109/15563650.2015.1115515
